Superficial Cervical Plexus Block
One of the few head and neck blocks that can done easily using either landmarks or ultrasound guidance.
Clinical indications: tympanomastoid surgery, ear surgery, cochlear implants, anterior neck/thyroid surgery, as an adjunct to clavicular surgery.
Techniques:
Ultrasound: In-plane approach
After sterile prep, place probe on the ipsilateral neck at level of cricoid cartilage (C6, roughly the middle of the SCM muscle)
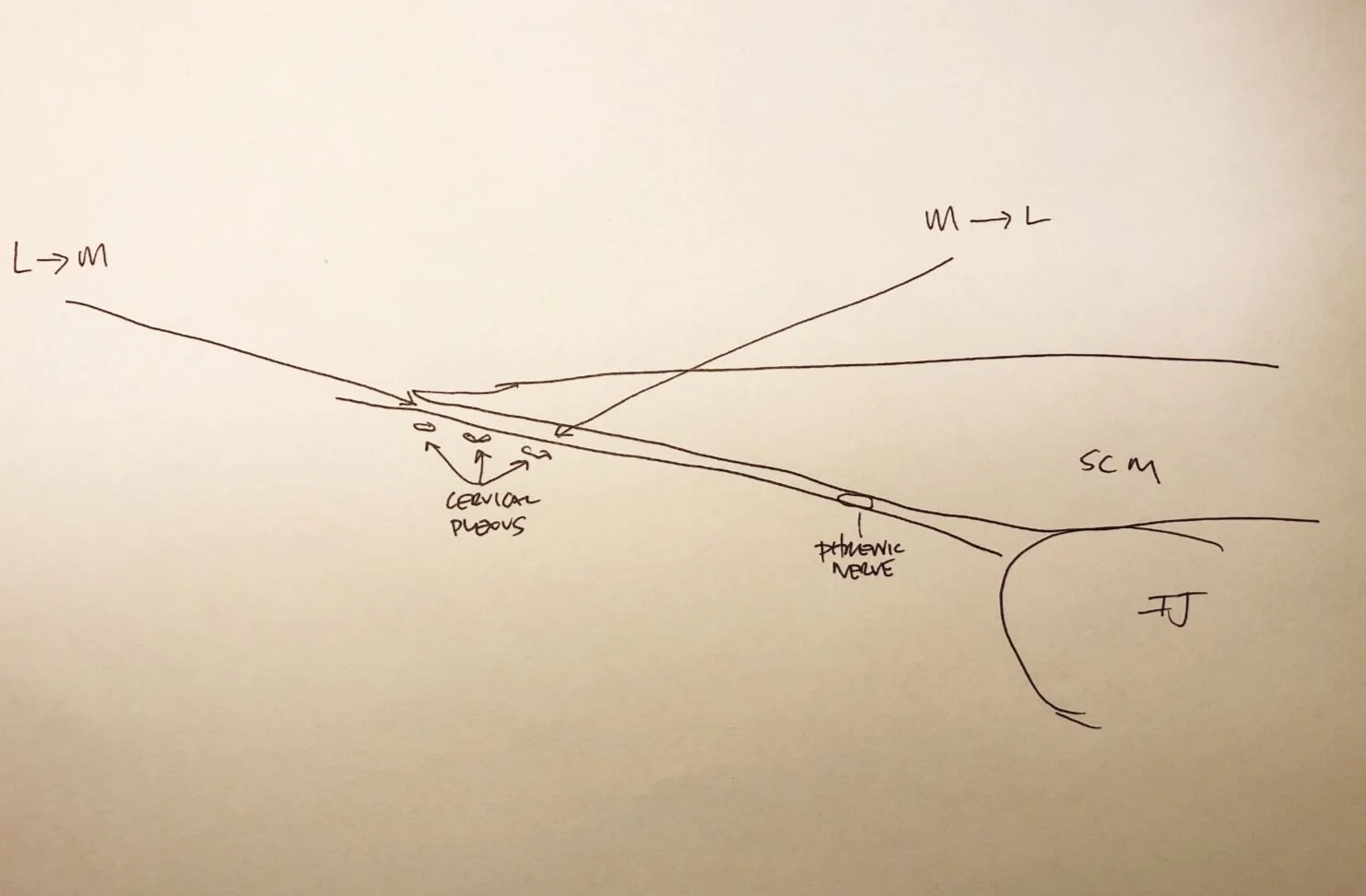
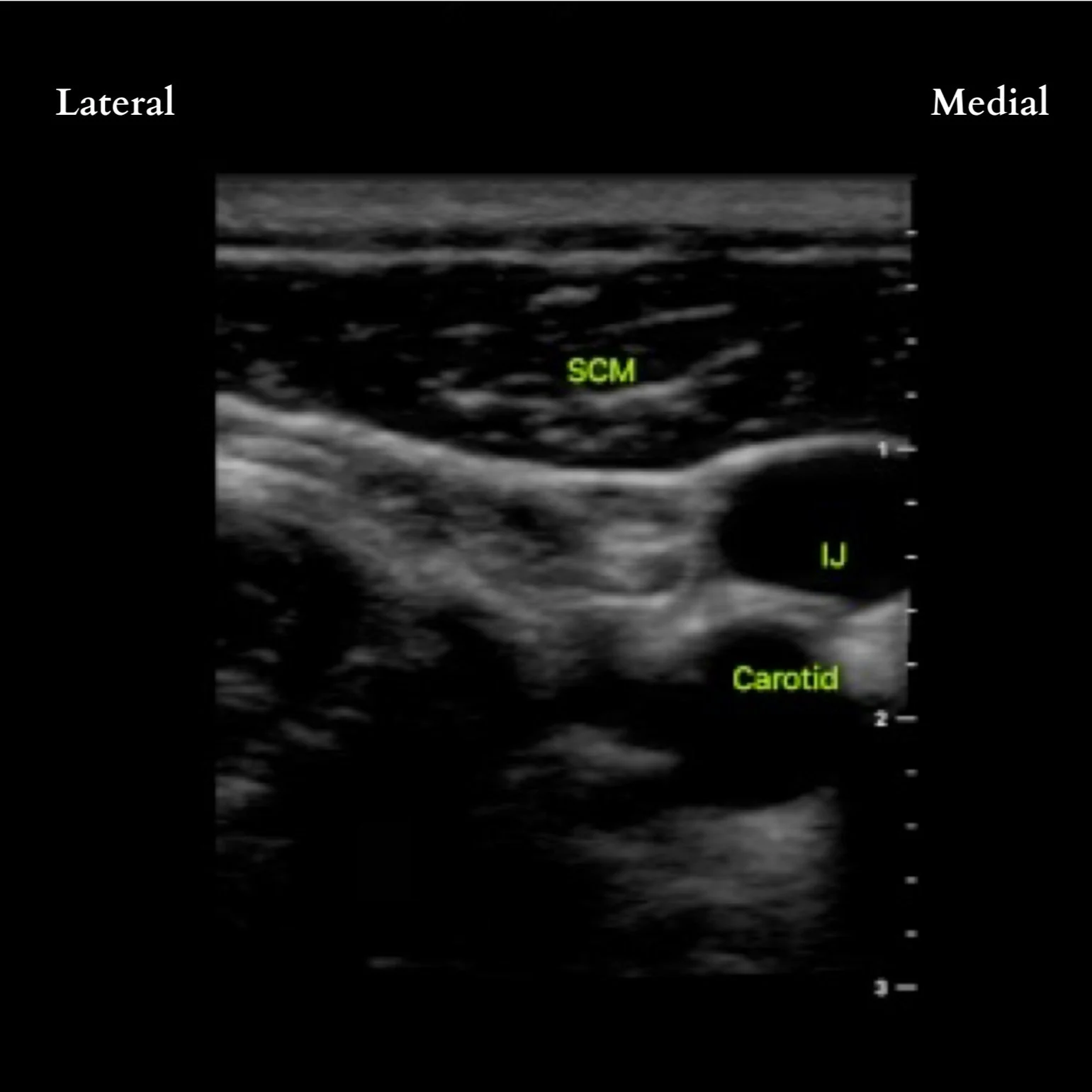
Moving the probe from medial to lateral, trace the SCM as it tapers laterally. If having trouble, first locate the great vessels. The SCM lies anteriorly.
If possible, identify the cervical plexus deep and posterolateral to the lateral edge of the SCM muscle as a hypoechoic collection of nodules. If not identifiable, LA can be deposited beneath the lateral edge of the SCM and prevertebral fascia. If in the correct plane, the LA will 'unzip' the layers similar to a TAP or rectus sheath block. Adjust needle tip accordingly to achieve this view. The phrenic nerve is routinely in this fascial plane (though deeper and medial), so ensure LA spread is more lateral and superficial to avoid unintentional phrenic nerve block.
Coverage: Anterior Rami of C2-C4 (sensory); a plexus comprised of 4 nerves: Lesser Occipital, Greater Auricular, Transverse Cervical and Supraclavicular.
Complications:
May interfere with intraoperative neuromonitoring if done pre-incision
Hematoma
Intravascular injection (presumably a higher incidence with landmark technique)
Potential Needle Paths
Phrenic nerve palsy (leading to ipsilateral diaphragmatic palsy)
The phrenic nerve is a mixed sensory/motor nerve with branches from C3-C5
Possible increased risk of post-operative fever (associated with B/L blocks and possible B/L phrenic nerve palsy, diaphragmatic palsy and atelectasis)
Can easily be ruled out using M-mode evaluation of the diaphragm.


Dillane, D., Ozelsel, T. and Gadbois, K., 2014. Anesthesia for clavicular fracture and surgery. Regional anesthesia and pain medicine, 39(3), p.256.
Tran, D.Q., Dugani, S. and Finlayson, R.J., 2010. A randomized comparison between ultrasound-guided and landmark-based superficial cervical plexus block. Regional anesthesia and pain medicine, 35(6), pp.539-543.
Merdad, M., Crawford, M., Gordon, K. and Papsin, B., 2012. Unexplained fever after bilateral superficial cervical block in children undergoing cochlear implantation: an observational study. Canadian Journal of Anesthesia/Journal canadien d'anesthésie, 59(1), pp.28-33.
de Arzuaga, C.I.S., Sieiro, J.M.N., Zafra, O.S., Posada, M.A.G. and Martínez, E.M., 2017. Selective Low-Volume Nerve Block for the Open Surgical Fixation of a Midshaft Clavicle Fracture in a Conscious High-Risk Patient: A Case Report. A&A Case Reports, 8(11), pp.304-306.