PEricapsular Nerve Group (PENG) Block

Indications: Hip fractures, Femoral neck fractures, Developmental dysplasia of the hip, Open & Arthroscopic hip surgery
Technique: Probe – Linear, Hockey Stick; Needle – In-plane
The child is placed supine in a neutral position.
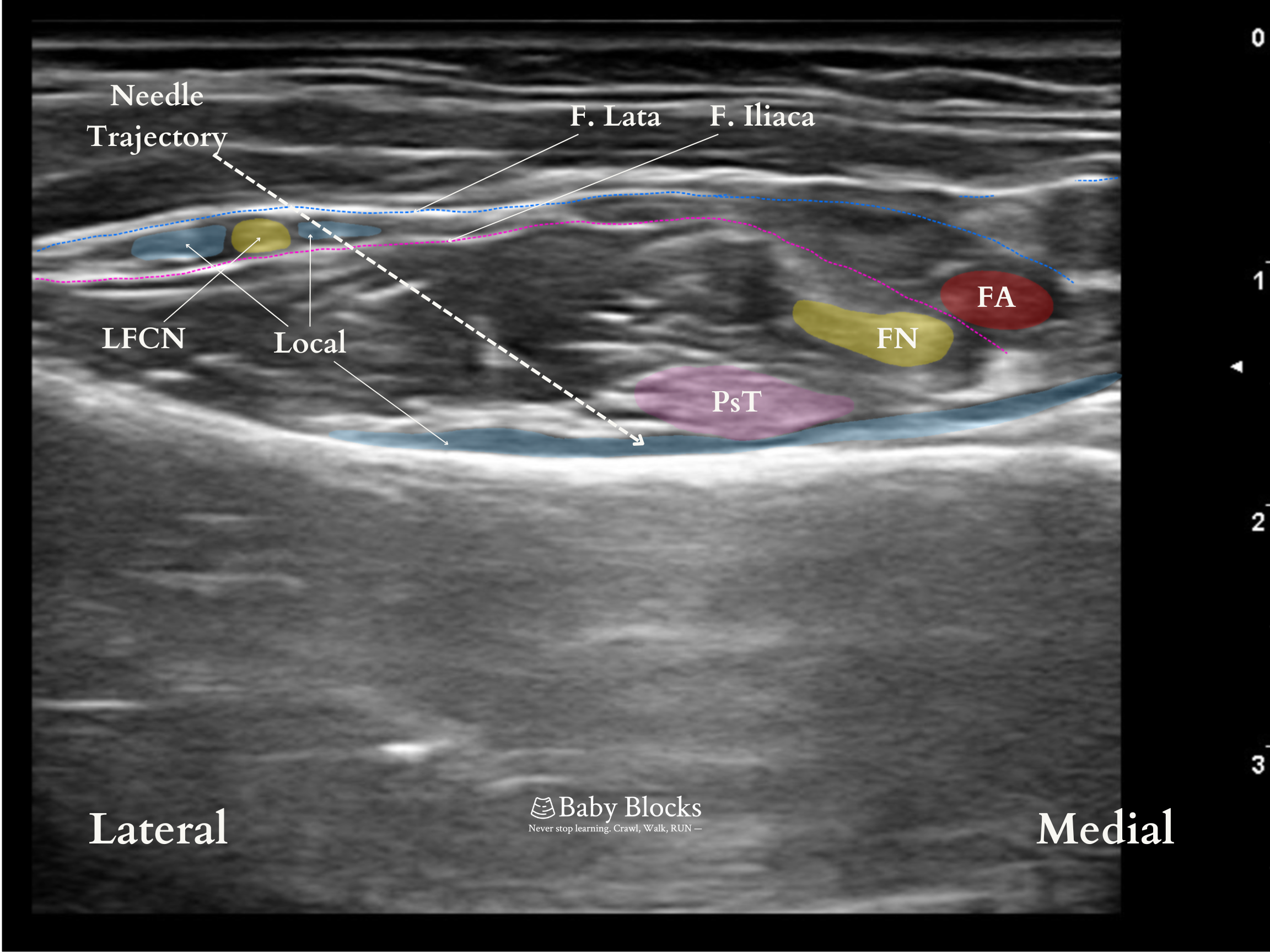
A linear ultrasound probe is positioned above the AIIS and rotated about 45 degrees in the direction of the pubic ramus. The femoral artery, pectineus muscle, and iliopsoas muscle and the psoas tendon are visualized.
A slight caudal tilt can be beneficial both for creating a better distance between the psoas tendon and femoral artery and nerve; and also for distribution of local anesthetic more caudally and directly to the sensory branches.
The needle is advanced from the lateral to the medial region using the in-plane approach. The area for the injection is between the pubic ramus and the psoas tendon. The local anesthetic is administered gradually once the fascia under the psoas tendon has been crossed and a negative aspiration test has been completed.
Linear spread above pubic ramus. The psoas tendon should be pushed up during injection.
Dose: 0.3 - 0.5ml/kg (maximum 20 mL) 0.25% bupivacaine or 0.2% ropivacaine
Coverage: Anterior hip capsule. The lateral thigh requires separate lateral femoral cutaneous coverage. A fascia iliaca block may be required if blockade of both the femoral and lateral femoral cutaneous nerves (LFCN) is desired. A small space on the medial thigh, just above the knee, requires obturator nerve coverage.
Potential Complications: Quadriceps muscle weakness, bladder injury, LFCN injury.
Tips:
Bone growth may not be completed until puberty, resulting in unique anatomical characteristics not found in adults, leading to different sonoanatomy. Malformations such as developing hip dysplasia should also be taken into account.
There have been reports of quadriceps weakness; however, an incorrect local anesthetic injection may be the source of this problem.
The local anesthetic has to be administered after going through the fascia underneath the psoas tendon. However, especially in youngsters, it may be difficult to insert a blunt-tipped block needle through this tissue immediately above the bone. Penetration can be made easier if needed by exerting rotating force on the needle with the thumb and index finger.
Because of the proximity to the bladder, it is not advisable to move the needle from medial to lateral.
The LFCN could be seen in the same view. While removing the needle, it can be blocked without requiring another puncture after completing the PENG block.
Patient Positioning and Probe Orientation
L: Lateral, M: Medial, Cr: Cranial, Ca: Caudal
Anatomy



Ultrasound Images

In hip surgery, adequate analgesia without the onset of the motor block has long been a goal, which has led to the continuous quest for peripheral regional anesthetic approaches. Giron-Arango et al defined the PENG block in 2018 to achieve this goal for anterior hip operations. The PENG block, which might be regarded as one of the most recently described fascial plane blocks, is also emerging as an alternative to lumbar plexus block (LPB) in children undergoing hip surgeries. While LPB is a deep and advanced block, the PENG block can be easily applied superficially and has begun being shown to be effective in hip surgeries. Recent studies emphasized the efficacy and simplicity of PENG block and described it as feasible for pain originating from the hip.
The articular branches of the obturator nerve, accessory obturator nerve, and femoral nerve innervate the anterior part of the hip capsule, the most pain-sensitive part of the hip joint because of its extensive innervation. The femoral and accessory obturator nerves' articular branches lie between the iliopubic eminence (IPE) and the anterior inferior iliac spine (AIIS), whereas the obturator nerve articular branches are at the inferomedial portion of the acetabulum. The delivery of local anesthetic to the subpectineal space—the area between the pubic ramus and the psoas tendon—guarantees that the local anesthetic will reach these branches. The motor block is not expected because the local anesthetic could not reach the femoral nerve as they are in different anatomical layers.
Bilateral PENG block could be applied to patients as the local anesthetic volume can be limited to 0.3-0.5 ml/per side. In addition, continuous PENG block after catheter placement is shown in the literature for adult patients. However, there is no data for the pediatric age group.
Girón-Arango L, Peng PWh, Chin KJ, Brull R, Perlas A. Pericapsular nerve group (PeNG) block for hip fracture. Reg Anesth Pain Med 2018;43:859–863
Yu HC, Moser JJ, Chu AY, Montgoery SH, Brown N, Endersby RVW. Inadvertent quadriceps weakness following the pericapsular nerve group (PENG) block. Reg Anesth Pain Med 2019;44:611–613.
Aksu C, Cesur S, Kus A. Pericapsular Nerve Group (PENG) block: Controversial points about anatomical differences. J Clin Anesth. 2020;61:109701
Aksu C, Cesur S, Kuş A. Pericapsular nerve group block and lateral femoral cutaneous block with single needle entry are possible in pediatric patients. J Clin Anesth. 2021;71:110215.
Anido Guzmán JA, Robles Barragán FJ, Funcia de la Torre I, Alfonso Sanz F, Becerra Cayetano IA, de la Hoz Serrano C. Bilateral pericapsular nerves group (PENG) block for analgesia in pediatric hip surgery. Rev Esp Anestesiol Reanim (Engl Ed). 2022;69:502-505.
Yörükoğlu HU , Cesur S , Aksu C , Kus A. B432 Opioid sparing effect of PENG block in open reduction of pediatric developmental dysplasia of the hip: a case series. Reg Anesth Pain Med 2022;47(Suppl 1):A288.