Interscalene Brachial Plexus Block
Coauthored with Carine Foz
Indications: Shoulder and upper arm surgery; Surgery of the distal clavicle (proximal clavicle can also be covered when combined with a Superficial Cervical Plexus Block)
Coverage: Brachial Plexus – Roots level
Considerations: Inferior trunk (C8-T1) is usually spared unless specifically targeted. This trunk corresponds to the ulnar nerve and its consequent coverage. Large volume local may spread to epidural space, phrenic nerve (hemidiaphragmatic paralysis); dorsal scapular nerve (winged scapula and impaired ability to elevate arm above the horizontal) or long thoracic nerve injury (winged-scapula). This is why Feigl et al advocate for an OOP technique, though they also caution to be mindful that the vertebral artery may be very superficial.
Patient position: Supine vs. Semi recumbent “beach-chair” vs. Lateral decubitus position; Neck turned to contralateral side. One can place a folded blanket or other padding between the shoulder blades to improve ergonomics for better anatomical exposure and needle insertion
Technique: Probe - Linear, Needle - In-plane (21, 22 or 25G echogenic needle for single shot) Appropriate needle with catheter for a continuous catheter technique.
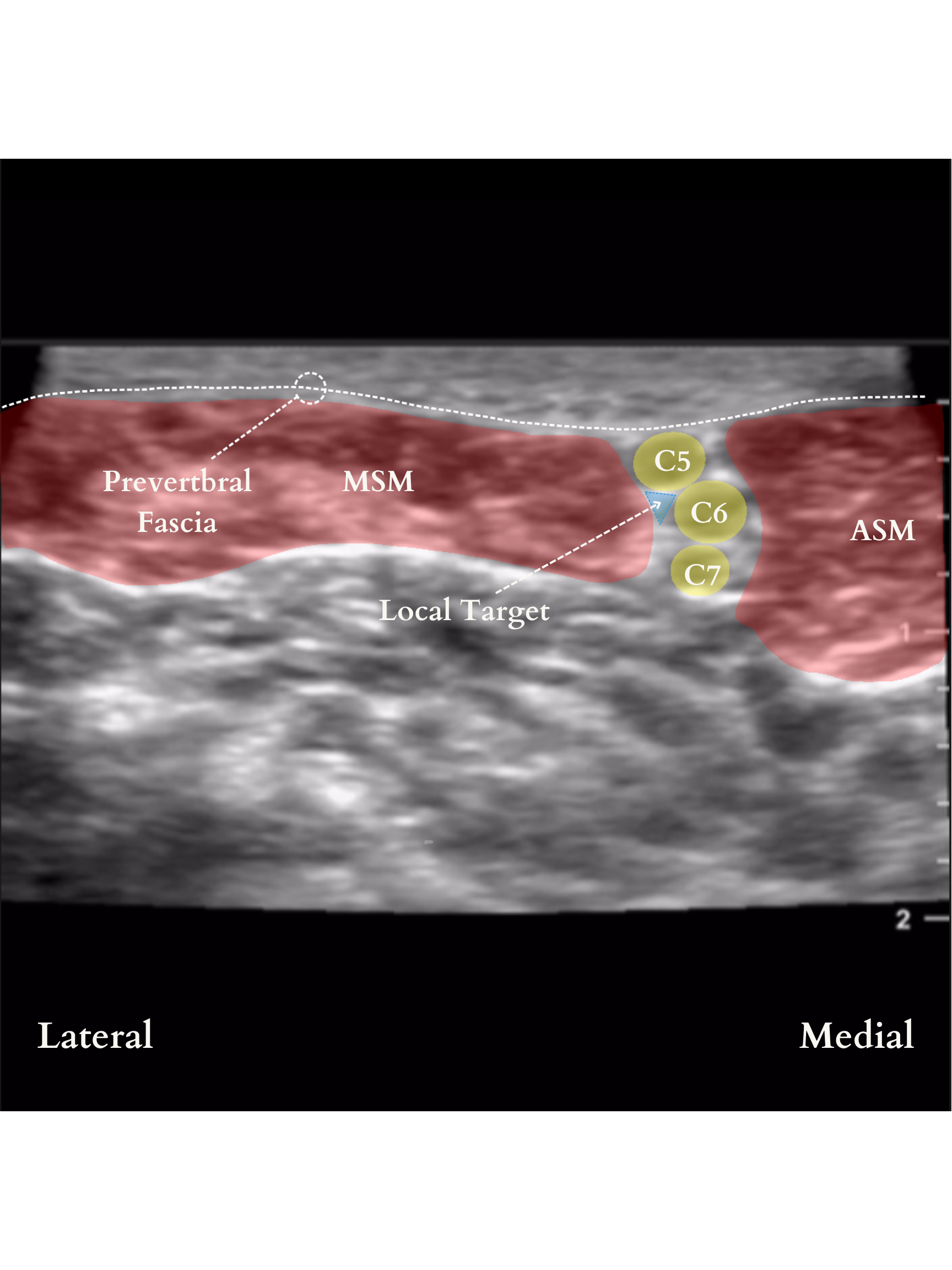
The posterior approach is considered the safest since the major vessels, nerves and sympathetic ganglia are anterior. It is also popular for ease of approach. In the classical approach, the ultrasound probe is placed over the sternocleidomastoid muscle at the level of the cricoid cartilage (transverse process of C6), between the anterior and the middle scalene muscles until the roots of C5, C6, and C7 are identified as three round hypoechoic spheres “traffic light sign”.
A common way to confirm the correct sonoanatomy is to place the probe in the supraclavicular fossa to identify the subclavian artery and the brachial plexus in what is referred to as the “bundle of grapes” sign. The probe is then translated in a cephalad direction keeping the nerves in view until the roots of C5, C6, and C7 are identified between the anterior and middle scalene muscles. A paper by Franco et al suggests that while the “traffic light sign” usually has 3 “lights,” they may in fact be made up of only 2 nerves (C5 and a split C6). The important clinical implication is that “an injection attempted between what is commonly perceived as the gap between C6 and C7 would indeed be an intraneural injection at C6, which could potentially spread toward the neuraxial space.”
As such, needle insertion is in plane targeting the pre-fascial space near the C5 and C6 nerve roots.
Another common way to identify the Brachial Plexus at the level of the Interscalene Groove is to trace the anterior rami of individual cranial nerves. As mentioned above, this may help identify instances where the three visible nerve roots are actually C5 and a split C6 (as captured in the video below!)




Dosing
Ropivacaine 0.2% with a volume of 0.25-0.5 mL/kg to a maximum of 25mL can be injected in small aliquots with intermittent aspirations to make sure that the needle tip did not migrate intravascularly
Ropivacaine 0.35% can also be used when a denser block is needed (a max dose of 2.5mg/kg)
Additives like dexmedetomidine, clonidine, or dexamethasone can also be added if a longer duration block is desired
Considerations
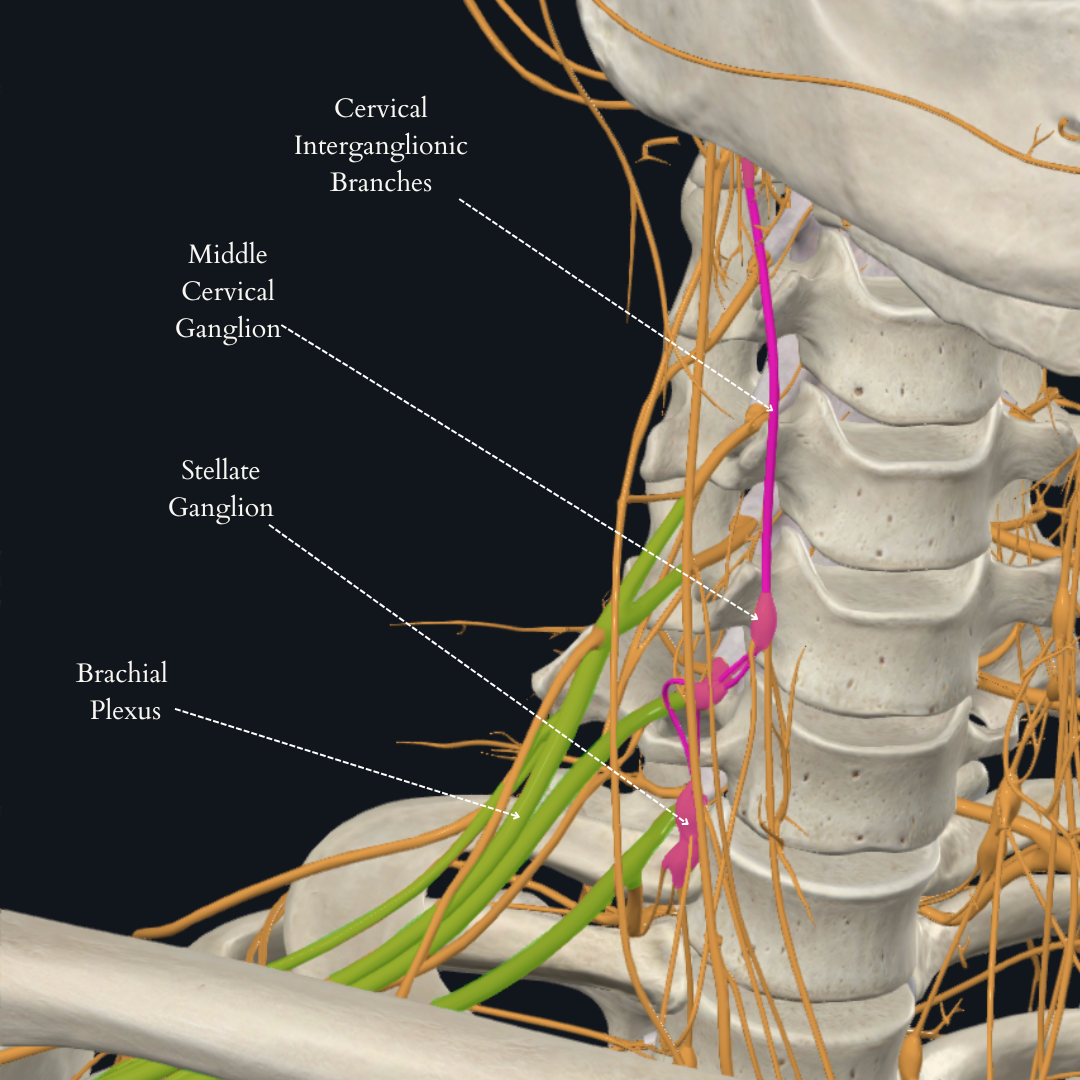
Horner’s syndrome (local anesthetic spread to cervical sympathetic chain)
Hoarseness (unclear etiology, though may be related to inadvertent blocking of phrenic and recurrent laryngeal nerves)
Ipsilateral hemidiaphragm (inadvertent blockade of the phrenic nerve)
Complications
Subarachnoid, epidural, or vertebral artery injection



Positioning, Probe Orientation & Sensory Loss
Positioning & Probe Orientation
Expected Sensory Loss
Ultrasound Images










Major shoulder surgery is characterized by severe acute postoperative pain necessitating a multidisciplinary approach to achieve effective multimodal analgesia. Inadequate postoperative pain control can lead to prolonged hospital stays, delayed recovery times, increased costs, as well as an increased risk of developing chronic shoulder pain. Regional anesthesia has had a significant impact on perioperative outcomes in orthopedic surgery including improved postoperative analgesia and rehabilitation, reduced opioid requirements, shortened hospital length of stay, and better functional outcomes and range of motion.
The use of interscalene brachial plexus regional techniques has been studied in the pediatric population. In a retrospective study, Aminian et al found a single-shot block to be a safe and effective method of providing superior postoperative analgesia and minimizing inpatient hospital admissions. They found that there was a statistically significant reduction in the pain scores within the first six hours of inpatient hospital admission in patients who received an interscalene nerve block when compared to those who did not (p = 0.0350). Moreover, 79% of patients who received a combined general and regional anesthetic technique were discharged home on the day of surgery, versus 45% who did not receive the block (P=0.036). Interscalene brachial plexus catheters have also been studied. Holland et al advised for the use of interscalene catheters in adolescent ambulatory shoulder surgery; they found it to be beneficial in terms of providing effective intraoperative and early postoperative analgesia.
With lower pain scores, minimal adverse events and and minimal opioid use, the use of an interscalene regional technique is advised for appropriately selected pediatric patients.
Mariano, E.R., Afra, R., Loland, V.J., Sandhu, N.S., Bellars, R.H., Bishop, M.L., Cheng, G.S., Choy, L.P., Maldonado, R.C. and Ilfeld, B.M., 2009. Continuous interscalene brachial plexus block via an ultrasound-guided posterior approach: a randomized, triple-masked, placebo-controlled study. Anesthesia and analgesia, 108(5), p.1688.
Feigl, G.C., Litz, R.J. and Marhofer, P., 2020. Anatomy of the brachial plexus and its implications for daily clinical practice: regional anesthesia is applied anatomy. Regional Anesthesia & Pain Medicine, 45(8), pp.620-627.
Kapral, S., Greher, M., Huber, G., Willschke, H., Kettner, S., Kdolsky, R. and Marhofer, P., 2008. Ultrasonographic guidance improves the success rate of interscalene brachial plexus blockade. Regional Anesthesia & Pain Medicine, 33(3), pp.253-258.
Franco, C.D. and Williams, J.M., 2016. Ultrasound-guided interscalene block: reevaluation of the “stoplight” sign and clinical implications. Regional Anesthesia & Pain Medicine, 41(4), pp.452-459.
Orebaugh, S.L., 2009. Ultrasound-guided regional anesthesia and pain medicine. Lippincott Williams & Wilkins
Beh ZY, Osman A, Fathil S, Karmakar MK. Ultrasound guided interscalene brachial plexus block with low dose sedation - Technique of choice for reducing shoulder dislocation. Am J Emerg Med. 2018;36(4):717-8.
Rafael Contreras M, Alejandro Ortega-Romero, MD. Ultrasound-guided interventional procedures for cervical pain. TECHNIQUES IN REGIONAL ANESTHESIA AND PAIN MANAGEMENT 17. (2013)64–80.
Erica Holland DL, Viviana Bompadre, Michael Saper. Continuous interscalene catheters for ambulatory shoulder surgery provide effective intraoperative and early postoperative analgesia in adolescent patients. BMJ. 2020;5:208–212.
Ahmet Eroglu, A case of transient hoarseness caused by interscalene brachial plexus block in shoulder surgery, BJA: British Journal of Anaesthesia, Volume 109, Issue eLetters Supplement, 31 December 2012
Kwater AP, Hernandez N, Artime C, de Haan JB. Interscalene Block for Analgesia in Orthopedic Treatment of Shoulder Trauma: Single-Dose Liposomal Bupivacaine versus Perineural Catheter. Local Reg Anesth. 2021;14:167-78.
Cozowicz C, Poeran J, Memtsoudis SG. Epidemiology, trends, and disparities in regional anaesthesia for orthopaedic surgery. Br J Anaesth. 2015;115 Suppl 2:ii57-67.
Egol KA, Forman J, Ong C, Rosenberg A, Karia R, Zuckerman JD. Regional anesthesia improves outcome in patients undergoing proximal humerus fracture repair. Bull Hosp Jt Dis (2013). 2014;72(3):231-6.
Dana Marie Aminian M, Tarun Bhalla, MD, Kelly Sprague, APN, Walter Samora, MD, Diane Von Stein, MD, Joseph D. Tobias, MD. A retrospective review of interscalene nerve blockade for shoulder surgery in the pediatric population. Anaesthesia, Pain & Intensive Care. 2014; VOL.18 NO.4.
Created in with collaboration with Physician Consultants of Soar-7