Deep Parasternal Intercostal Plane Block


Indications: Sternotomy, Pectus Carinatum repair, medial rib fractures or breast procedures
Special Considerations: The internal thoracic vessels reside in the injection plane and should be avoided. The block is also done within millimeters of the pleura, so the needle tip should always be visualized. Thankfully, in younger children, the ultrasound actually penetrates through cartilage, thus reducing the acoustic shadow’s “blind spot.”
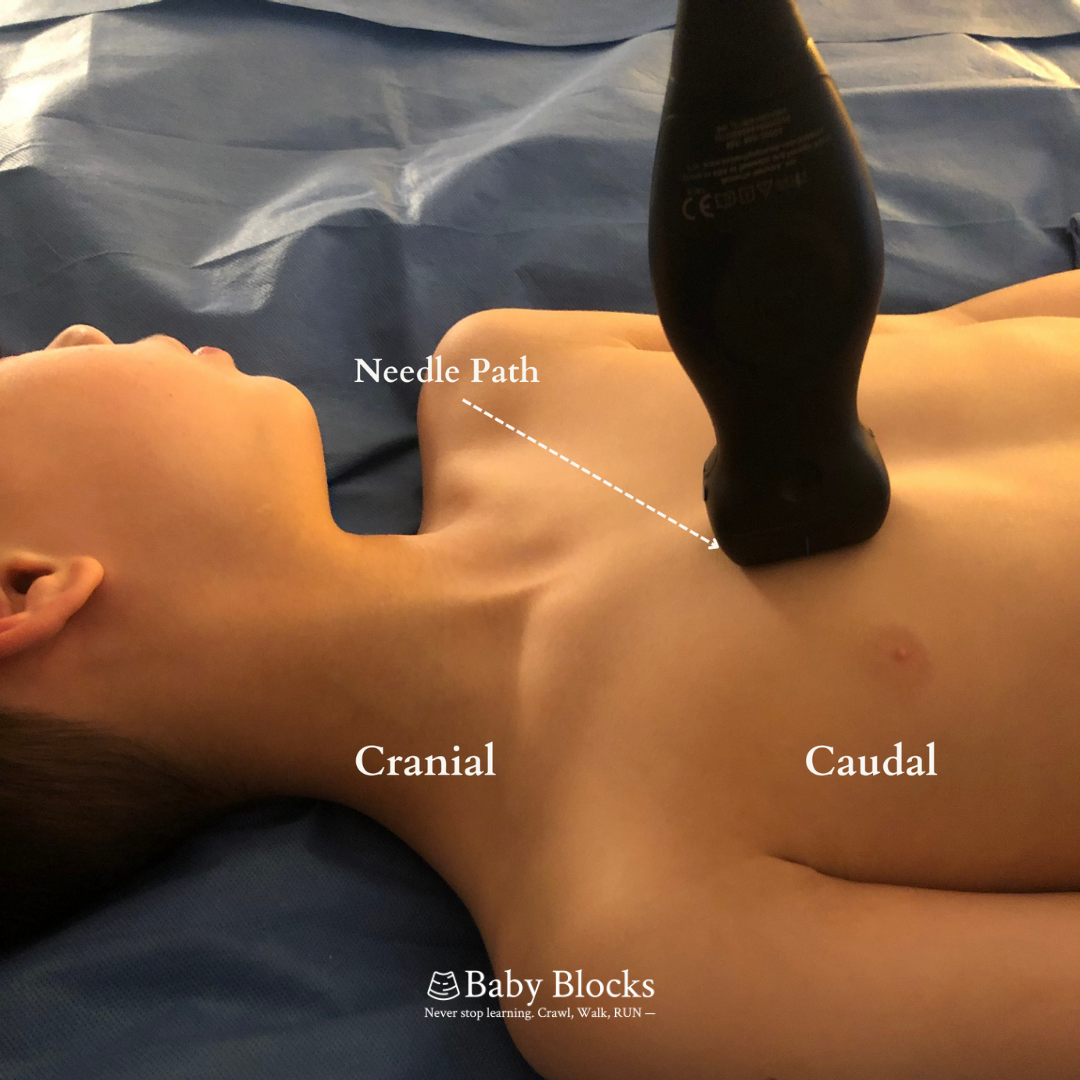
Patient Position: Typically supine, but may be done with patient in full lateral (as long as one has access to anterior chest, position is a balance between convenience and circumstance).
Technique: In-plane, parasagittal; though can be done in-plane, transverse if concerned about internal thoracic vessels
Coverage: T2-T6 anterior cutaneous nerves (green highlighted region)
Potential Complications: Hematoma, IMA injury, pleural puncture, pneumothorax, pericardial puncture, hemopericardium & cardiac injury.
Patient Positioning, Probe Orientation & Sonoanatomy







Originally described in 2015, the Transversus Thoracic Muscle Plane Block—as it was initially called—has had a bit of a whirlwind introduction to the world, not the least of which is a brand new name! As many of you know, a recent ASRA/ESRA collaboration set out to standardize nomenclature based on anatomical features in an effort to reduce the rapid expansion of largely duplicative regional techniques. As such, the TTP block has been re-christened the Deep Parasternal Intercostal Plane block, or Deep PIP Block for short.
While much of the initial controversy surrounding the validity of the Deep PIP block has been more thoroughly and independently verified by other researchers and publications, there still remains some ongoing debate as to whether we should be doing this block at all. In addition to the general risks of any regional technique, the Deep PIP block has some unique factors that shouldn’t be taken lightly. First, the needle tip is intentionally advanced to within millimeters of a beating heart and sliding lungs. As such, this block is obviously not for the faint of (cough cough) heart! (Sorry). Secondly, the needle also passes through the same plane as the internal mammary artery, the gold-standard conduit for patients undergoing CABG surgery. Any or all of those structures may be unintentionally injured while performing a deep PIP block.
Most of the available evidence on the deep PIP block happens to be in adults, and even that evidence is typically case series or small RCTs. In the two RCTs in kids that I could find, a sum total of 87 kids received deep PIP blocks for cardiac surgery. No complications were found. In a follow-up retrospective study by one of the original RCT teams, Abdelbaser et al looked at almost 200 pediatric patients (6 mos. to 18 years old) over a 32-month period who had pre-incisional deep PIP blocks prior to cardiac surgery. In their study, they had (1) hematoma, (1) pleural puncture, and (1) pericardial puncture, each with an estimated incidence of 0.5%. The hematoma “was not related to internal mammary vessels but was self-limiting and spontaneously resolved.” The pericardial and pleural punctures were both incidentally noted after sternotomy, neither of which caused any untoward events or required any further intervention. The authors attribute the punctures to “the loss of sonographic visualization of the needle tip during needle advancement and the low experience of the physician who performed the block.” There were no injuries to the IMA vessels, pneumothorax, hemopericardium or cardiac injury observed.
Is the deep PIP block the only block routinely performed where one risks injuring such vital structures? Absolutely not.
While there is nothing nearly as robust as the PRAN database to fall back on for reassurance when performing a deep PIP block, the risk of iatrogenic pneumothorax while performing a PVB block is still estimated at around 0-1% . There are also case reports of pneumothorax associated with both deep serratus and ESP, (though the ESP case report has since been retracted for obvious reasons). While many practitioners would argue that there is a much safer alternative to the deep PIP block, namely the superficial PIP block, from a technical perspective the superficial is nearly identical to the deep serratus and ESP. In all three, one aims for the muscle layer overlying either the rib or transverse process that itself overlies the pleura.
With the exception of location, at least in my mind, these three blocks (superficial PIP, deep serratus, and ESP) are basically identical in technique and probably risk for iatrogenic pneumothorax. Having said that, I will readily concede that the risk of pneumothorax should theoretically be higher in the deep PIP as compared to the superficial. I think a more suitable comparison, looking at both technique and what evidence is out there, is that the risk associated with performing the deep PIP block is probably much closer to a PVB, though time will tell.
As for vascular injury, as this block has typically been done in cardiopulmonary bypass cases for congenital cardiac lesions, such as intracardiac shunts, it remains unclear what long-term effects unintentional injury to the internal thoracic artery may play for patients requiring a coronary bypass procedure perhaps decades in the future. My suspicion is that the risk is very low. Also, with the ultrasound already in hand, one can typically identify vascular structures either grossly or with the addition of color doppler. And if one is still unsure, rotating the probe from parasagittal to transverse may also help identify the vessels and aid in both avoidance, as well as hydrodissection of the correct plane. At one point in time, we recommended piercing arteries while performing blocks!
Having touched on some of the idiosyncratic risks of the deep PIP block, are there any potential benefits when compared to the superficial? Perhaps. One possible advantage of the deep PIP is that one injection typically achieves a unilateral multidermatomal block (T2-T6). While I was unable to find explicit evidence of the superficial PIP requiring multiple injections due to difficulty of hydrodissection, a number of colleagues who routinely perform both the superficial and deep say they often find that to be the case.
In the end, both techniques offer similar analgesic efficacy (especially if one takes into account the confounding impact of unilateral ITA harvesting on injectate spread). While the deep PIP may offer the possibility of a single injection, it does come with a higher price: potentially higher risk of injury to important structures.
One thing does seem clear no matter which one you perform, viewing the needle tip throughout the procedure is paramount. A plan A block this is not!
Ahiskalioglu, A., Kucun, T., Yayik, A.M., Ulas, A.B. and Ates, İ., 2021. Ultrasound-guided transversus thoracis muscle plane block provides effective postoperative analgesia for pediatric open pectus carinatum surgery: first report. Pain Medicine, 22(5), pp.1233-1235.
El-Boghdadly, K., Wolmarans, M., Stengel, A.D., Albrecht, E., Chin, K.J., Elsharkawy, H., Kopp, S., Mariano, E.R., Xu, J.L., Adhikary, S. and Altıparmak, B., 2021. Standardizing nomenclature in regional anesthesia: an ASRA-ESRA Delphi consensus study of abdominal wall, paraspinal, and chest wall blocks. Regional Anesthesia & Pain Medicine, 46(7), pp.571-580.
Walker, B.J., Long, J.B., Sathyamoorthy, M., Birstler, J., Wolf, C., Bosenberg, A.T., Flack, S.H., Krane, E.J., Sethna, N.F., Suresh, S. and Taenzer, A.H., 2018. Complications in pediatric regional anesthesia: an analysis of more than 100,000 blocks from the pediatric regional anesthesia network. Anesthesiology, 129(4), pp.721-732.
Zhang, Y., Chen, S., Gong, H. and Zhan, B., 2020. Efficacy of bilateral transversus thoracis muscle plane block in pediatric patients undergoing open cardiac surgery. Journal of Cardiothoracic and Vascular Anesthesia, 34(9), pp.2430-2434.
Abdelbaser, I.I. and Mageed, N.A., 2020. Analgesic efficacy of ultrasound guided bilateral transversus thoracis muscle plane block in pediatric cardiac surgery: A randomized, double-blind, controlled study. Journal of Clinical Anesthesia, 67, p.110002.
Abdelbaser I, Mageed NA. Safety of Ultrasound-Guided Transversus Thoracis Plane Block in Pediatric Cardiac Surgery: A Retrospective Cohort Study. J Cardiothorac Vasc Anesth. 2021 Dec 10:S1053-0770(21)01063-6
Desai, M., Narayanan, M.K. and Venkataraju, A., 2020. Pneumothorax following serratus anterior plane block. Anaesthesia reports, 8(1), pp.14-16.
Winnie AP. Does the transarterial technique of axillary block provide a higher success rate and a lower complication rate than a paresthesia technique? New evidence and old. Reg Anesth. 1995 Nov-Dec;20(6):482-5. PMID: 8608065.
Liu, V., Mariano, E.R. and Prabhakar, C., 2018. Pecto-intercostal fascial block for acute poststernotomy pain: a case report. A&A Practice, 10(12), pp.319-322.
Kaya C, Dost B, Dokmeci O, Yucel SM, Karakaya D. Comparison of Ultrasound-Guided Pectointercostal Fascial Block and Transversus Thoracic Muscle Plane Block for Acute Poststernotomy Pain Management After Cardiac Surgery: A Prospective, Randomized, Double-Blind Pilot Study. J Cardiothorac Vasc Anesth. 2021 Oct 1:S1053-0770(21)00837-5.