Ankle Block

Indications: Foot/toe surgery
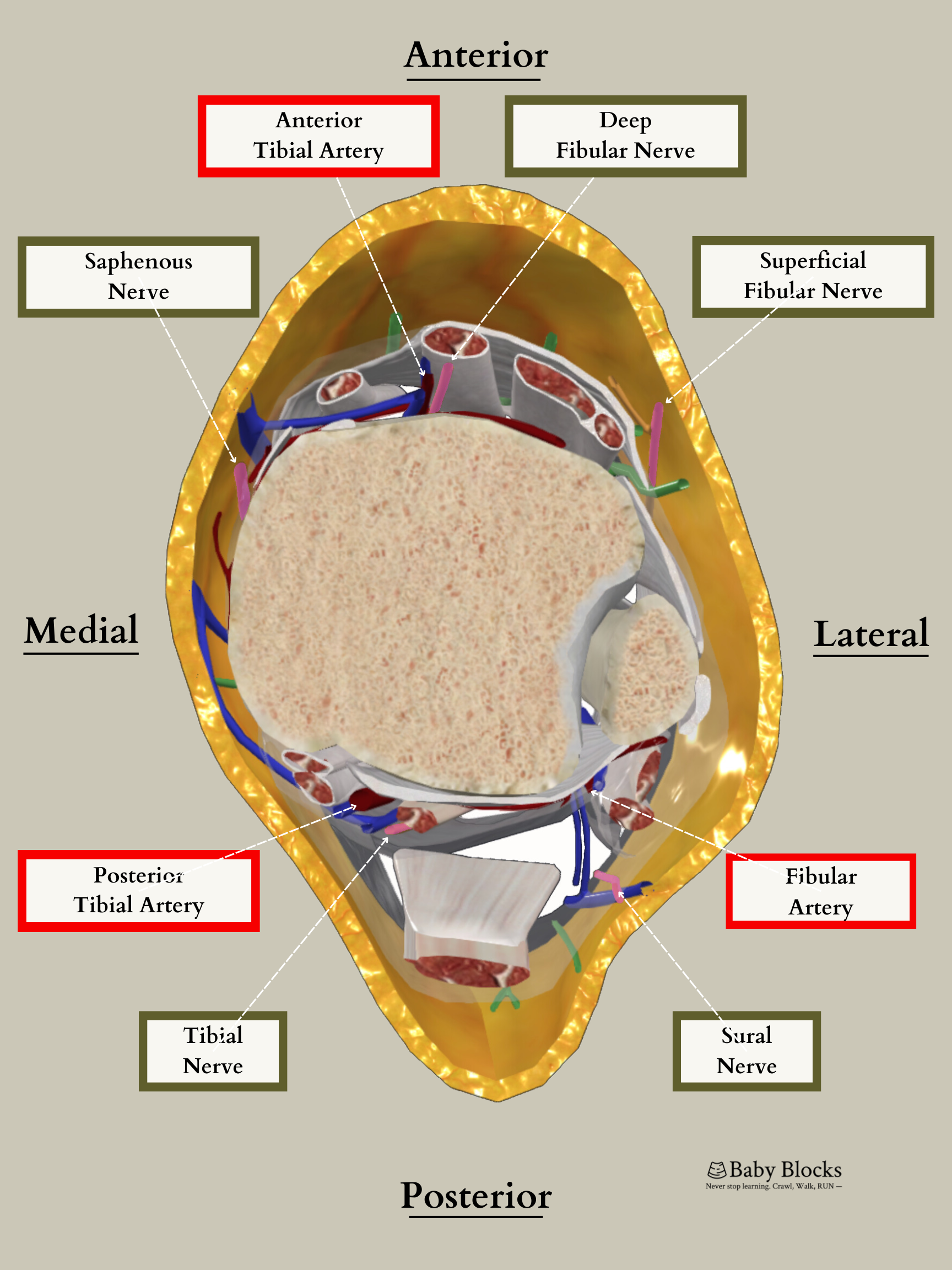
Anatomy
Saphenous nerve: medial shin/ankle onto foot towards big toe
Sciatic nerve:
Tibial nerve: heel through bottom of foot
Deep fibular nerve: webspace between big toe and second toe
Superficial fibular nerve: front of shin/ankle onto top of foot through all toes
Sural nerve: lateral shin/ankle onto foot towards pinky toe
Dose: 0.5 - 1.5mg/kg of Bupivacaine or Ropivacaine (roughly 0.2 - 0.3mL/kg).
Coverage: Anterior thigh, anteromedial knee, and anteromedial lower leg to the level of the medial malleolus.
The lateral thigh requires separate lateral femoral cutaneous coverage. A fascia iliaca block may be required if blockade of both the femoral and lateral femoral cutaneous nerves is desired. A small space on the medial thigh, just above the knee, requires obturator nerve coverage.
Motor function to the quadriceps muscle group will be affected. If a sensory block to the knee or below, without motor involvement, is required an adductor canal block or more distal saphenous nerve block can be utilized.
Potential Complications:
If using landmark technique the subcutaneous injection of local on the anterior aspect of the ankle to block the saphenous and superficial fibular nerves has caused skin breakdown.
Inadequate blockage of surgical and/or tourniquet pain requiring either supplemental local, supplemental sedation, and/or general anesthesia.
Low risk for infection, bleeding, neuropraxias.
Technique:
Landmark:
Typically, I aim to block the tibial nerve first by palpating the tibial artery posterior to medial malleolus and inserting the needle, avoiding the artery, until bone is contacted. Then local anesthetic is spread in a fan-like manner since the nerve may be posterior or anterior to the artery.
Next target is the deep fibular nerve which is blocked by palpating the anterior tibial artery on anterior ankle between extensor hallucis longus and extensor digitorum longus tendons. The needle is inserted, avoiding artery, until bone is contacted, and local anesthetic is injected in a fan-like manner.
Then the saphenous nerve is blocked by injecting local anesthetic subcutaneously while moving medial towards the medial malleolus from the insertion site for the deep fibular nerve block.
The superficial fibular nerve is blocked by injecting local anesthetic subcutaneously in the same manner from the same starting point but in the lateral direction.
Lastly the sural nerve is targeted by inserting the needle cephalad and posterior to the lateral malleolus until bone is contacted and injecting local anesthetic while withdrawing the needle.
Ultrasound-Guided:
When utilizing ultrasound for the ankle block keep in mind that the nerves are very small and often it is much easier to identify the vasculature nearby or other anatomical landmarks.
Tibial Nerve
Linear probe parallel to the sole of foot posterior to medial malleolus to visualize tibial artery and nerve. Needle placed out of plane to deposit local anesthetic circling nerve.



Saphenous Nerve
Linear probe parallel to sole of foot anterior to medial malleolus (this can be accomplished by moving anterior from the position of the problem for the tibial nerve) to visualize the great saphenous vein which runs with the saphenous nerve. Needle can be placed in plane or out of plane to surround the neurovascular bundle.



Deep Fibular Nerve
Linear probe on anterior ankle perpendicular to tibia to visualize anterior tibial artery and deep fibular nerve. Needle can be inserted in plane or out of plane to deposit local anesthetic around nerve.



Superficial Fibular Nerve
Linear probe placed on lateral ankle perpendicular to fibula a few finger breaths above lateral malleolus to visualize nerve between peroneus brevis and extensor digitorum longus muscles superficially. Needle should be inserted in plane from anterior to posterior to surround nerve. (Figure 4)



Sural Nerve
Linear probe placed on lateral ankle parallel to sole of foot posterior to medial malleolus (this can be accomplished by moving distally towards the lateral malleolus and posteriorly from the position of the probe for the superficial fibular nerve) to visualize the sural nerve running with the short saphenous vein. Needle can be inserted in plane to surround the neurovascular bundle.



Traditionally, anesthesia residents were taught to use a landmark technique for ankle blocks that involved multiple injection sites and high volumes of local anesthetics. Unfortunately, this approach was often quite painful for patients and only provided sensory, not motor, block, which meant it couldn't prevent patients from moving due to surgical stimulation. In my training, I found that these blocks worked best for elderly patients with existing neuropathy who didn't need much sedation.
These factors have led to a decline in the use of ankle blocks, especially in pediatric patients! However, ankle blocks do offer some advantages, which can be valuable for pediatric patients. For instance, patients with an ankle block can bear weight on the blocked foot, which is easier than keeping a young child non-weight bearing after a popliteal block makes their foot numb. The increased use of US guidance for block placement has also allowed a significant decrease in the required volumes of local anesthetic which may also make ankle blocks a more attractive option for pediatric anesthesiologists.
Albaqami, Mohammed S and Adel A Alqarni. "Efficacy of Regional Anesthesia Using Ankle Block in Ankle and Foot Surgeries: A Systematic Review." European Review for Medical and Pharmacological Sciences (2022): 471-484.
Brown, David L, et al. Atlas of Regional Anesthesia. Philadelphia, PA: Saunders Elsevier, 2010.
Chan, Vincent WS, et al. Ultrasound Imaging for Regional Anesthesia: A Practical Guide. Toronto, ON: Toronto Printing Company, 2009.
Chin, Ki J, et al. "Ultrasound-guided Versus Anatomic Landmark-guided Ankle Blocks: A 6-year Retrospective Review." Journal of Regional Anesthesia & Pain Medicine (2011): 611-618.
Delbos, Alain, et al. "Ultrasound-guided ankle block. History revisited. ." Best Practice & Research Clinical Anaesthesiology (2019): 79-93.